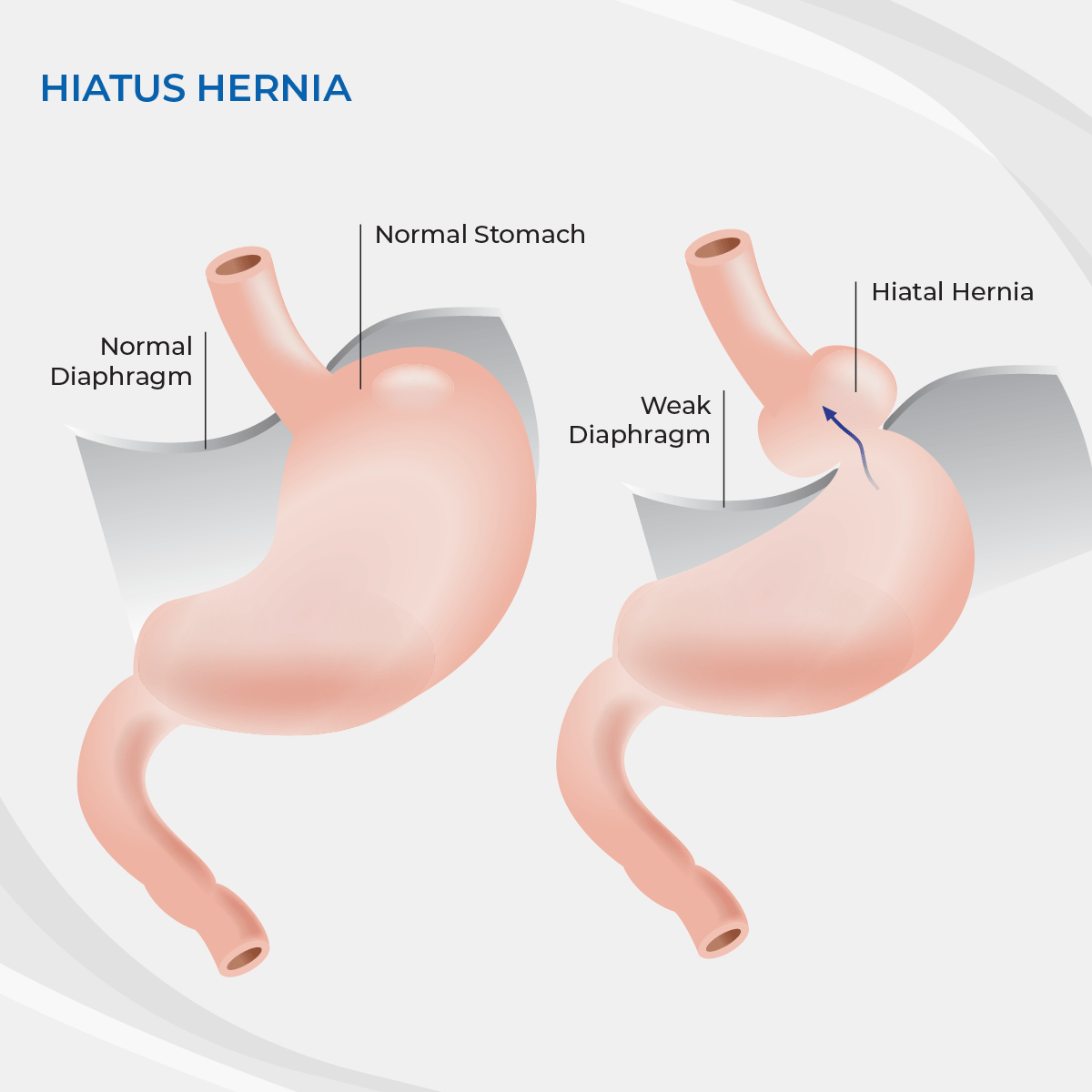
Hiatus hernia is a condition where all or part of your stomach slips or ‘herniates’ through your diaphragm into your chest. A lot of people have smaller hernias which don’t need fixing, but larger hernias can give you significant problems.
Problems your hernia may cause you include
- symptoms of reflux such as burning or an acid taste in your mouth
- iron deficiency anaemia from ulcers caused by your stomach rubbing on your diaphragm (from its abnormal position)
- shortness of breath or poor exercise tolerance (caused by the slipped stomach pressing on the heart and impairing its ability to pump blood and oxygen around the body)
- chest pain
- difficulty swallowing,
- cough, worsening of your asthma
- occasionally the stomach can twist or ‘volve’ requiring emergency surgery.
Operation
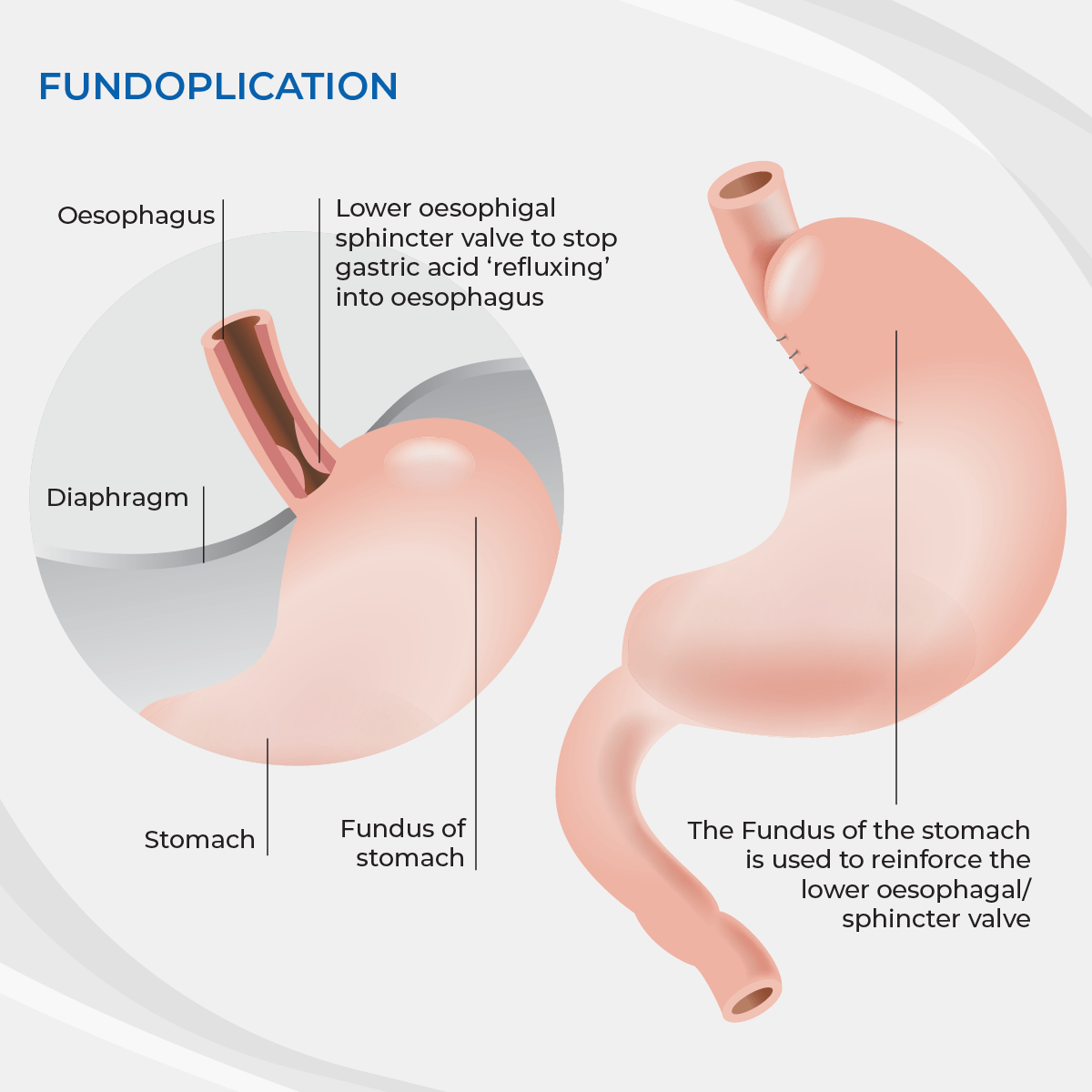
A hiatus hernia can effectively treated by an operation called laparoscopic hiatus hernia repair. This is a key hole operation to return the stomach to its normal position and tighten the hole in the diaphragm that it slipped through. As part of your operation Dr Hamer will usually perform a partial fundoplication (anti-reflux operation) to both help reflux symptoms, but also to help prevent your stomach from slipping back into your chest. Laparoscopic hiatus hernia repair is an operation requiring a general anaesthetic and usually a 2 night stay in hospital.
Side effects to be aware of
All operations have side effects or potential complications you need to be aware of. Risks of any operation include the risk of the anaesthetic, small risks of bleeding, infection and hernias developing in the key hole entry sites. Specific to hiatus hernia repair you need to know that your surgeon is operating in the area of blood vessels called the aorta and the vena cava, nerves which help the stomach to empty, the oesophagus, stomach, liver and spleen. Although injuries to these are rare, they can occur.
Longer term the hernia can sometimes reoccur. If this does happen, in most people it doesn’t occur as severely as it did the first time, doesn’t cause as many symptoms and usually doesn’t need another operation.
After the fundoplication part of the operation, some people can have difficulty swallowing. This is usually temporary and gets better as the swelling from the operation goes down. Occasionally further treatment may be necessary. As the fundoplication tightens the valve between the stomach and oesophagus it can effect how the stomach and bowel process wind. About 20-30% of people find that they get wind symptoms after fundoplication. This can be ‘gas-bloat’ syndrome where you feel bloated, have difficulty with belching or vomiting, or get increased flatulence.
Non operative treatment
You have the option of continuing with anti-reflux medication and making lifestyle modifications to try and manage your symptoms. This is not successful in everyone.
What to expect
You will be admitted to the hospital on the day of your operation. You will meet the nursing staff and the anaesthetist who will be administering your anaesthetic. After your operation you will wake up in the recovery area of the hospital where specialized recovery nurses will look after you and ensure you recover from your anaesthetic safely. After this you will be moved either to the ward. At any stage if the nurses have concerns about your recovery they will contact your anaesthetist or Dr Hamer. After waking up from your operation you will initially be allowed water to drink. After this you will be allowed to try some food of a pureed consistency.
After your operation
Diet:
You will need to be careful with what you eat after your hernia repair. For the first month you should eat only very soft foods that don’t require a lot of chewing. You should avoid bread, red meat and pasta. You should avoid fizzy drinks during this period. After a month you can slowly start trialing a normal healthy diet again. If you are having trouble with any particular food, simply stop and try again in a week or two.
Anti-reflux medications:
After your operation you should be able to come off your anti-reflux medications. Immediately after your operation you should continue taking them for 4 week, then slowly wean yourself off. If you come off too quickly you may find that some of your symptoms temporarily recur. If this happens, start taking them again, but try coming off them slowly again in a couple of weeks.
Dressings:
After you have been discharged from the hospital, you will have dressings over your wounds. These do not affect how well your wounds heal, but they do protect your clothes from any seepage which may occur. If they become dirty or wet they may simply be removed and changed for a similar dressing or a band aid. After a week they can be removed and discarded. Occasionally people feel more comfortable leaving a dressing on for an extra week, particularly if the wound is somewhere that can rubs on your clothing.
Sutures:
Your wounds will be closed with either glue or dissolving sutures, neither need removal.
Pain killers:
Most people find taking regular paracetamol to be enough for their pain. Paracetamol has the advantage (unlike most other pain killers) that it won’t make you constipated or feel woozy. It is also very safe if taken carefully according to the instructions on the packet. In some circumstances you will be given additional pain killers to take home with you. If this is the case you should read and follow the instructions carefully.
Problems:
Complications are unusual. If you do have any problems you have multiple ways of accessing help. During office hours you can contact Dr Hamer’s rooms or your GP. For more pressing problems or after hours you can also contact the emergency department at the hospital.
Recovery:
Generally most people find that they are fit to return to light duties at work after 1 -2 weeks. You should avoid heavy lifting for four weeks after your operation. If you are still having significant problems at this time you should be reviewed to ensure you are still recovering properly.
Follow Up
You will be reviewed 4-6 weeks after your operation to ensure you have recovered.